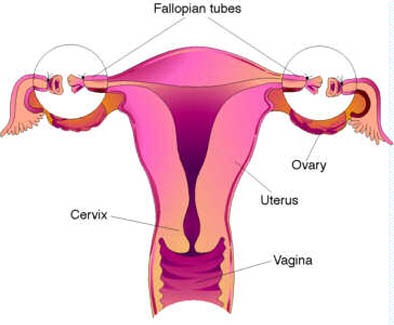
Tubal ligation (incorrectly referred to as tubectomy). Typically requiring the patient to undergo local, general, or spinal anesthesia. It is advised that women should not undergo this surgery if they currently have or had a history of bladder cancer. After the anesthesia takes effect, a surgeon will make a small incision at each side of, but just below the navel in order to gain access to each of the two fallopian tubes. With traditional tubal ligation, the surgeon severs the tubes, and then ties (ligates) them off thereby preventing the travel of eggs to the uterus. Other methods include using clips or rings to clamp them shut, or severing and cauterizing them. Tubal ligation is usually done in a hospital operating-room setting.
Effectiveness
A tubal ligation is approximately 99% effective in the first year following the procedure. In the following years the effectiveness may be reduced slightly since the fallopian tubes can, in some cases, reform or reconnect which can cause unintended pregnancy. Method failure is difficult to detect, except by subsequent pregnancy, unlike with vasectomy or IUD.